
.png)
Frozen shoulder is significantly more common in women during perimenopause and menopause because declining oestrogen reduces anti-inflammatory and ant...
.png?width=1376&height=768&name=9bc04e3e-fe06-4586-b91d-8c504e8dddb7%20(1).png)
Frozen shoulder is significantly more common in women during perimenopause and menopause because declining oestrogen reduces anti-inflammatory and anti-fibrotic protection in shoulder tissues. Treatment combines physiotherapy, pain management, and potentially menopausal hormone therapy (MHT).
If you've noticed a persistent ache in your shoulder that worsens at night, or found yourself unable to reach behind your back, you're not imagining things. Frozen shoulder — medically known as adhesive capsulitis — is a common but often under-recognised symptom of menopause. It affects women between 40 and 60 at a far higher rate than any other group, and the timing is no coincidence. The hormonal changes of perimenopause and menopause play a direct role in how and why shoulder tissue becomes inflamed and scarred. This article explains the connection, what to expect as the condition progresses, and the full range of treatment options available.
Table of Contents
- What Is Frozen Shoulder?
- The Oestrogen-Shoulder Connection
- The Three Stages of Frozen Shoulder
- Risk Factors That Increase Your Chances
- How Frozen Shoulder Is Treated
- Can Hormone Therapy Help?
- Lifestyle Support for Joint Health
- Frequently Asked Questions
- Conclusion
What Is Frozen Shoulder?
Frozen shoulder occurs when the capsule of connective tissue surrounding the shoulder joint becomes inflamed, thickened, and scarred. As this capsule tightens, it restricts the shoulder's normal range of motion — sometimes dramatically. The result is a shoulder that feels literally "frozen," painful to move, and frustrating to live with.
The condition affects roughly 2-5% of the global population, but the demographics are striking: three-quarters of those diagnosed are women, and the peak incidence falls squarely between ages 40 and 60 — the perimenopausal and menopausal window [1].
Frozen shoulder is now recognised as part of the broader 'musculoskeletal syndrome of menopause' — the collective burden of joint pain, muscle loss, bone density changes, and connective tissue deterioration driven by oestrogen decline [1]. More than 70% of women experience musculoskeletal symptoms during the menopause transition, and around 25% will find them significantly disabling [1].
The Oestrogen-Shoulder Connection
Oestrogen does far more than regulate the menstrual cycle. It actively maintains joint, tendon, ligament, and connective tissue health throughout the body — including the shoulder capsule. When oestrogen levels fall during perimenopause, these protective effects weaken.
How Oestrogen Protects the Shoulder
Oestrogen works in several ways to keep shoulder tissue healthy:
- Anti-inflammatory: Oestrogen helps regulate inflammatory responses. Without it, the shoulder capsule becomes susceptible to the low-grade chronic inflammation that initiates frozen shoulder.
- Anti-fibrotic: Oestrogen suppresses fibroblasts — the cells that produce scar tissue. When oestrogen declines, this suppression is lost and fibrosis of the shoulder capsule accelerates.
- Collagen regulation: Oestrogen influences collagen synthesis and breakdown. Its decline reduces capsule elasticity and promotes stiffening [2].
- Joint lubrication: Oestrogen supports the synovial membrane, which produces lubricating joint fluid. Less oestrogen means more friction and stiffness.
Indirect Effects of Menopause
Menopause also affects frozen shoulder through secondary pathways. Sleep disorders, anxiety, and depression — all common during the menopause transition — are independently associated with increased shoulder pain sensitivity and slower recovery. Systemic inflammation linked to hormonal imbalance can compound localised joint inflammation, making symptoms feel more intense and longer-lasting.
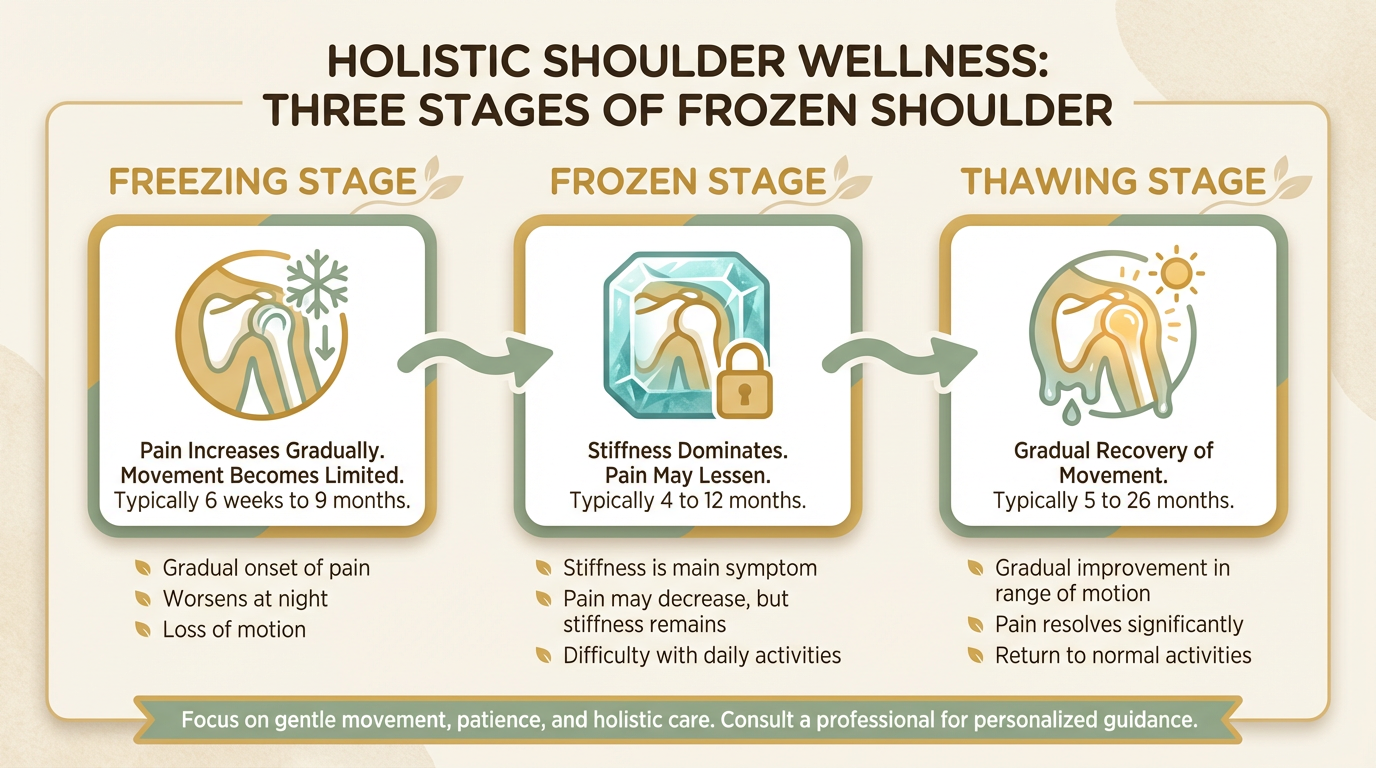
The Three Stages of Frozen Shoulder
Understanding the stages helps you know what to expect and why treatment needs to adjust at each phase.
Stage 1: Freezing (6 weeks to 9 months)
The most painful stage. Shoulder discomfort begins gradually — often mistaken for a muscle strain — and night pain is a hallmark. Many women are woken by shoulder pain when rolling over in bed. Range of motion progressively diminishes.
Stage 2: Frozen (4 to 6 months)
Pain may ease, but stiffness becomes the dominant problem. The shoulder loses significant range of motion, making everyday tasks — fastening a bra, reaching a shelf, putting on a jacket — genuinely difficult.
Stage 3: Thawing (months to years)
Mobility gradually returns and pain continues to reduce. Full recovery can take several months to a few years. Physiotherapy during this stage significantly accelerates return to function.
Tip: Don't wait until Stage 2 to seek help. Early intervention in the freezing stage — particularly corticosteroid injections and guided physiotherapy — can reduce the severity and duration of the condition.
Risk Factors That Increase Your Chances
While oestrogen decline is a significant factor, frozen shoulder is multifactorial. Women in the perimenopausal and menopausal years face heightened risk if they also have:
- Diabetes: People with diabetes have a 10-20% rate of frozen shoulder, compared to approximately 2-5% in the general population. This is the strongest known risk factor.
- Thyroid disorders: Both hypothyroidism and hyperthyroidism are associated with elevated risk.
- Previous shoulder injury or surgery: Immobility following injury or a procedure can trigger the inflammatory cascade.
- Cardiovascular disease or stroke: These conditions increase the likelihood of shoulder complications.
- A sedentary lifestyle or prolonged immobility: Lack of regular shoulder movement can contribute to capsular thickening.
If you have any of these factors alongside perimenopausal or menopausal symptoms, joint pain or new shoulder stiffness warrants early assessment.
Shoulder pain alongside other menopause symptoms? A menopause-focused doctor can assess the hormonal picture and help you build the right treatment plan. Book a bulk-billed consultation — no referral needed.
How Frozen Shoulder Is Treated
There is no single treatment that resolves frozen shoulder — effective management usually involves a combination of approaches tailored to your stage and symptom severity.

Physiotherapy
Guided physiotherapy is typically the cornerstone of treatment. A physiotherapist will design a graduated programme of range-of-motion and stretching exercises appropriate to your stage. Gentle, structured movement — rather than forcing through pain — is the key principle, particularly in the freezing stage. Self-directed stretching without guidance can sometimes worsen inflammation.
Corticosteroid Injections
Intra-articular corticosteroid injections are recommended in the earlier stages when inflammation is high. Research suggests they reduce pain and improve function, particularly in the first 12 weeks. They are most effective when combined with physiotherapy.
Pain Relief and Other Options
Non-steroidal anti-inflammatory drugs (NSAIDs) may help manage day-to-day pain. Hydrodilation — injecting sterile fluid to gently stretch the joint capsule — is an option for persistent cases. Surgery (arthroscopic capsular release) is reserved for severe cases unresolved after 12-24 months of conservative care.
Can Hormone Therapy Help?
This is a question many women ask, and emerging research suggests the answer may be yes — though it requires nuance.
A retrospective cohort study of 1,952 women aged 45-60 found that those not receiving menopausal hormone therapy (MHT) had 99% greater odds of a frozen shoulder diagnosis compared to those who did receive it [3]. Around 4% of MHT users were diagnosed, compared to nearly 8% of non-users [3]. The authors noted the study was underpowered and called for larger confirmatory investigations.
MHT is not currently prescribed as a direct frozen shoulder treatment. However, if you are experiencing other menopause symptoms — including hot flushes, muscle tension, fatigue, or mood changes — hormone therapy may address the underlying oestrogen deficiency that contributes to shoulder tissue vulnerability.
Body-identical hormone therapy using products listed in the ARTG is the preferred approach. Transdermal oestrogen has a more favourable safety profile than oral forms, and micronised progesterone is preferred over synthetic progestogens. Treatment is always individualised — your doctor will assess your full health history before making any recommendation.
Note: Hormone therapy is not suitable for everyone. Your doctor will assess whether it's appropriate for you based on your individual health history, symptoms, and risk factors. Individual results may vary.
Lifestyle Support for Joint Health
Alongside medical treatment, lifestyle measures can meaningfully support shoulder recovery and overall joint health during menopause.
- Movement: Regular, gentle activity — swimming, yoga, walking — maintains shoulder mobility and reduces systemic inflammation. Targeted shoulder strengthening supports joint stability.
- Nutrition: An anti-inflammatory diet rich in omega-3 fatty acids (oily fish, flaxseeds, walnuts) and colourful vegetables may help modulate the inflammatory processes driving frozen shoulder.
- Sleep and stress: Poor sleep amplifies pain perception. Addressing sleep disorders through better sleep hygiene or medical support helps the body's natural repair processes. Chronic stress elevates cortisol, compounding inflammation.
- Heat and cold therapy: Heat packs before movement and cold packs after exercise can ease discomfort between formal physiotherapy sessions.
Tip: A multidisciplinary approach works best. Combining physiotherapy with nutritional support, naturopathic care, and appropriate medical treatment addresses frozen shoulder from multiple angles simultaneously.
This information is for educational purposes only and is not medical advice. Consult your healthcare provider for personalised recommendations. Treatment decisions should be individualised based on your medical history and circumstances.
Explore the full range of menopause treatment options available through a specialist menopause service.
Frequently Asked Questions
Is frozen shoulder a symptom of menopause?
Frozen shoulder is not classified as a classic menopause symptom, but it is significantly more common during perimenopause and menopause. It is now considered part of the broader 'musculoskeletal syndrome of menopause', which describes the collective musculoskeletal effects of oestrogen decline [1].
How long does frozen shoulder last during menopause?
The full cycle typically lasts one to three years across all three stages, though this varies widely. Early treatment — particularly physiotherapy and corticosteroid injections — often shortens the course.
Can hormone therapy prevent frozen shoulder?
Preliminary research suggests MHT may reduce risk, with one study finding nearly half the diagnosis rate in MHT users versus non-users [3]. However, MHT is not currently approved as a preventive treatment, and the evidence needs confirmation in larger trials. Discuss the potential joint health benefit with your doctor if considering MHT for menopause symptoms.
What exercises help frozen shoulder in menopause?
Guided physiotherapy exercises are most effective — typically pendulum swings, cross-body stretches, and finger-walking exercises. Work within a pain-free range, particularly during the freezing stage, and always start with professional guidance to avoid worsening inflammation.
Conclusion
Frozen shoulder and menopause share a clear biological connection. Declining oestrogen weakens the anti-inflammatory and anti-fibrotic defences that protect shoulder tissue, making perimenopausal and menopausal women disproportionately vulnerable. The good news: frozen shoulder is treatable, and addressing both the local shoulder symptoms and the underlying hormonal picture offers the most complete path to recovery.
If you're experiencing shoulder pain, stiffness, or any other signs and symptoms of menopause, speaking with a menopause-focused clinician can help you understand the full picture. The Australian Menopause Centre has been supporting women through the menopause journey since 2003, with telehealth consultations available nationwide — no referral required.
References
- Wright, V. J., Schwartzman, J. D., Itinoche, R., & Wittstein, J. (2024). The musculoskeletal syndrome of menopause. Climacteric, 27(5), 466–472. https://doi.org/10.1080/13697137.2024.2380363
- Chidi-Ogbolu, N., & Baar, K. (2019). Effect of estrogen on musculoskeletal performance and injury risk. Frontiers in Physiology, 9, 1834. https://doi.org/10.3389/fphys.2018.01834
- Saltzman, E., Kennedy, J., Ford, A., Reinke, E., Green, C., Poehlein, E., & Wittstein, J. (2023). Poster 188: Is hormone replacing therapy associated with reduced risk of adhesive capsulitis in menopausal women? Orthopaedic Journal of Sports Medicine, 11(7_suppl3). https://doi.org/10.1177/2325967123s00174


